|
Welcome! Now that you've decided conditioning your baby that you will not respond so they give up and fall asleep on their own is NOT the way to go, what is the way? You don't have to stay stuck not knowing what to do about unsustainable sleep deprivation. Chronic sleep deprivation is the #1 cause of postpartum depression, which is not good for your baby and it's no wonder: You are doing the most important job in the world and you are physically and mentally debilitated by a basic essential need: your own sleep. There is a way through, without resorting to painful sleep training that sacrifices your baby's optimum emotional well being and security. My Smart Baby Sleep system will show you the way, including 6 months!! of ongoing support in my private group, Science Mommy Secure Line. Healthy sleep is on the way!
22 Comments
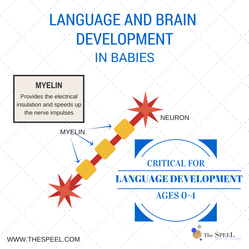
By Guest blogger, Alex Trichilo, Speach Pathologist at www.thespeel.com Speech Pathologists have long been aware of a critical period in baby language development, in which the brain develops rapidly and is capable of learning a LOT. What we have learned more recently is what changes are actually occurring in the brain to allow this to happen. Some recent research from 2013 from O’Muircheartaigh and colleagues that looks at brain white matter assymmetry changes in the brain in the early years and its relation to language and cognition is very exciting. This research was really the first of its kind and involved studying 108 children with typical development, ranging in age from one to six years. Being an early study in this area, it suggests that we can’t draw confident conclusions, but the results suggest some important future directions for research in this area. O’Muircheartaigh and his colleagues have continued to do more research in this area over the last few years. This study looks at the myelin that surrounds each nerve axon and how it develops from birth, and what they found was amazing! First of all, lets take a look at what myelin is: Myelin wraps around each nerve axon and is so important because it provides the electrical insulation and speeds up the nerve impulses. (See below for a graphic of how it looks.)
“The fastest lifetime rate of both expressive and receptive language acquisition occurs between 18 and 60 months” (p.16173, O’Muircheartaigh, 2013). This, together with the rapid myelin development, explains the amazing number of words that we see children develop at these ages, they move from only saying a few words or sounds to being able to hold entire conversations with adults. When children use and understand language on a regular basis, the brain typically learns to ‘lay down’ more myelin, which speeds up the impulses in the nerves and makes for a great foundation of language. It is important that we make the most of this incredible period of language development so that we can give children the best communicative opportunities in life. O’Muircheartaigh and his colleagues have continued to do more research in this area over the last few years.
Making the most of the critical period: Right from your child’s birth you can be doing many things to make the most of this critical period of language development. These include: · Monitoring your child’s hearing skills, especially if they regularly suffer from ear infections. · Taking the time to play and talk with your child one on one. · Turning the TV off when you are not watching it, avoid having it there as background noise · Praising your child and rejoicing in the development of new words together · Adding language to every day activities (bath time, play time, grocery shopping) If you feel that your child is not developing their communication skills from an early age, first head to www.thespeel.com to get the free printable checklist for your child’s age. If you continue to be concerned, get in touch with me, or contact a local Speech Pathologist. Enjoy the early years of language development and know that you are making an amazing difference in your child’s life by surrounding them with language opportunities.  Part 1 is a prelude to the following:
To varying degrees, a compromised first year of life is the norm, because factions of our society rail against any aspect of parenting seen as interfering with women’s career advancement. The ability to return to the workplace quickly and seamlessly is considered paramount. Child development advocates like Darcia Narvaez, PhD, argue that our values are due for a upgrade (see part one of this post). Should we sacrifice our careers somewhat for healthier children and a more compassionate society? Probably. But what if that sacrifice was only on the surface and short-lived? What if in the long run, the investment we make in our children through Narvaez's Evolved Developmental Niche (EDN) parenting strategies paid dividends at the individual, corporate, and societal levels? What if this investment in very early child development improved the productivity of nations, saved billions on healthcare costs, and even better equalized the gender gap in the workplace? The Projected Savings of High-Nurturing At the individual level, the benefits of extended breastfeeding and ample loving touch—the core of the EDN—are obviously palpable. We want to give these gifts to our babies. But the mental health savings of investing in the very early years (primarily the first year) can be as well, simply by considering the mental health crisis and among other things, the work of Allan N. Schore, PhD, who shows its roots in infancy. According to the U.S. Department of Health and Human Services, four million children and adolescents in the U.S. suffer from a serious mental disorder that causes significant functional impairments at home, at school, and with peers. Of children nine to 17 years old, 21 percent have a diagnosable mental or addictive disorder that causes at least minimal impairment. We’re given a convenient scapegoat for this, of course: darn genetics. But health crises don’t reach epidemic proportions because of genetics. Evolution happens through genes, but epidemics occur too quickly. There has to be something going on in the environment. In this case, in the emotional and social environment of the first year or so of life. (Read a presentation by Dr. Allan Schore about how early child rearing quality creates protection against versus risk for mental illness.) The Next-Generation Savings of High-Nurturing John Beddington, PhD, has extensively studied the “mental capital” of economies, which will prove vital to the future success of nations. Mental capital is defined as encompassing both cognitive and emotional resources, including, as he states: “flexibility and efficiency at learning; and emotional intelligence, social skills and resilience in the face of stress.” Beddington’s definition bears a striking resemblance to the outcomes of Narvaez’s EDN (discussed in Part One of this post): Higher social and emotional intelligence, better learning and memory capacities, stress resilience, and greater compassion and cooperation. In concert with Narvaez's assertions, the genetic contribution to the “mental capital” Beddington researches, by his own account, is well below 50 percent in childhood, and it’s only that high because of intelligence. Tease IQ out and the emotional and social capacities are even less genetically determined—hovering around 20-30 percent, if they exist at all. Even when looking at genes, as the burgeoning field of epigenetics reveals, we’re rarely looking only at genes: “Genes are themselves inert,” Narvaez states in her latest textbook, Neurobiology and the Development of Human Morality: “They do not act alone but require an interactive context of environmental influence, maturation, and action.” Add to that, even when a mentally detrimental gene gets activated by the environment, a change in that environment—such as, perhaps, receiving EDN-conducive parenting—can limit its influence on the child’s future mental well-being. Genes are not destiny. This is why biologically-informed parenting practices confer the best chance for optimal development of mental capital within any given set of genetics. This is especially true during the first year of life when the foundations of mental health and social and emotional capacities are forming. So, let’s look at the numbers to address the obvious question emerging: How much does mental illness cost us versus the investment in mental-health-promoting childhoods (i.e., the EDN)? The Substance Abuse and Mental Health Services Administration (SAMHSA) cites a cost of $150 billion for mental health care in the U.S., roughly equivalent to the cost of cancer care. (One third of this is eaten up by anxiety disorders.) And that’s just the cost of treatment. Without treatment, the consequences of mental illness for the individual and society are enormous. Unlike cancer, the economic burden of mental illness is not only the cost of care, but unemployment, absenteeism, substance abuse, homelessness, inappropriate incarceration, and a myriad of indirect costs due to chronic disability that begins early in life. According to the National Alliance on Mental Illness (NAMI), the economic cost of untreated mental illness is more than 100 billion dollars each year in the United States. The World Health Organization (WHO) has reported that four of the 10 leading causes of disability in the US are mental disorders. Something beyond genetics is happening here, just by virtue of the rate at which it’s getting worse. Depression across the U.S. is now between 10 and 20 times the rate it was 50 years ago while its average age of onset is a decade younger. We’re now up to $250 billion in costs. But due to another law of our biology—we can’t separate mind and body—the costs don’t stop with mental health. The contribution of early intense stress (i.e.: cry-it-out sleep training, touch deprivation, infant isolation) to later disease and degeneration has an astonishing effect on life-long productivity. This is too complex to assign a number, but one example of these effects provides a good starting point: The Journal of the American Medical Association recently reported that conditions in the U.S workplace such as arthritis, headaches, and back problems cost nearly $50 billion per year. These types of ailments are being increasingly linked to early, chronic childhood stress, as the work of Robin Karr-Morse exposes. But there are innumerable other diseases with stress correlations. The Immediate Savings of High-Nurturing We wouldn’t even need to wait a generation to begin realizing a hearty return on an EDN baby-rearing investment. More breastfeeding alone could save $26 billion per year in medical-care costs, based on the U.S. Department of Health and Human Services Office on Women’s Health (OWH) calculation of 90 percent of babies being breastfed exclusively for the first six months saving $13 billion; extended breastfeeding confers additional health savings. Caring for a sick child also enters the equation quickly in terms of current loss of productivity, because it takes the worker out of commission just as surely as the worker being ill herself does. Employee absences due to caring for sick children in the United States costs businesses approximately $3 billion dollars every year. While breastfeeding, especially the EDN’s exclusive and extended variety, reduces babies’ risks of virtually all infection and when a breastfed baby does become ill, he will typically recover far faster and with less medical intervention. Formula fed babies, on the other hand, are at increased risk for allergies, Type 1 and 2 diabetes, Crones disease, ulcerative colitis, dental cavities, certain types of cancers, including childhood lymphomas, and more. Since breastfed babies are statistically healthier than their formula fed peers, the parents of breastfed babies spend less time out of work and less money on health care. This point illuminates the need for not just longer maternity leave to improve breastfeeding rates, but better breastfeeding and pumping accommodations at work so moms don't have to sacrifice breastfeeding to maintain their careers. Much of the opposing debate has centered on what breastfeeding costs in terms of short term career productivity, but even the study much cited to assert this breastfeeding blame suggests the solution isn't less breastfeeding, but rather more workplace accommodations. The study authors note: "Should breastfeeding be shown to have a negative impact on work outcomes, our study will provide evidence that breastfeeding promotion needs to be coupled with protections for women's work and earnings". Such protections would really benefit the company, too, even beyond lower health care costs. This is because even if we manage to get enough quality baby care to go back to work at 12 weeks post partum, how much are we really able to give to our jobs in that dizzying first year? The corporate problem of workers reporting in while not well (for a variety of reasons) has become so financially detrimental that the term “presenteeism” was coined to describe it. Presenteeism is defined as the practice of employees not operating to their usual level of productivity due to illness or extreme fatigue. Could there be a better exemplar for this than the first year of parenthood? We’re only human, not machines, and as biology dictates—neither are our babies. They demand what they need and our jobs gets what’s left of our energy—or vice-versa, and then we’re back to an increased mental health risk. The total cost of presenteeism to U.S. employers has been increasing; estimates for current company losses range from about $150 to $250 billion annually. Depression alone set U.S. employers back some $35 billion a year in reduced performance at work, not counting when depression takes them out of work (absenteeism). So how much savings from the presenteeism problem could an EDN-based society enjoy? The National Women’s Law Center estimates that women giving birth represent 1.6 percent of the workforce. We’ll double that figure to count the father in the equation (3.2 percent of 200) since, if he’s pulling his weight in the post-partum months, he’s suffering from presenteeism too. This equals a cost of just over six billion dollars attributable to baby-induced presenteeism alone. Adding both the immediate and future savings outlined above, let’s calculate how much of that $332 billion could be saved with child rearing closer to what nature intended. This is a conservative approach, not fully weighing in the percentage of immeasurable costs attributable to chronic physical illness (other than mental) at an additional $500 billion. If at least 70 percent of child mental health is determined by early parenting practices (on average, 30 percent is “genetic” [note limitations of this stat above]), and the EDN is correlated with better mental health outcomes, then let’s say the EDN-experience for all babies could cut future mental disorders by 70 percent. Let’s use the same percentage for just those several ailments know to be tied to mental health (although we know most others are, too), plus the whole $26 billion in savings for breastfeeding and six billion from presenteeism, for a total of around $242 billion. Alternatively, some combination of longer leave, flexible work hours, and higher quality childcare conducive to the “multiple caregivers who are all bonded to baby” element of the EDN could help realize similar savings. Now, how does this compare to the short-term cost of a more reasonable six-to-12 month paternal leave (divided between two parents)? Leave it to breastfeeding advocate, KellyMom, to calculate a figure of $113 billion for one year of leave paid at 75 percent of the mom’s normal wages, for all mothers. (Since men earn slightly more, the cost to share leave with dads would be around ten percent higher, though better for the economy as detailed below.) So considering the costs, investing in support that allows for the EDN would pay for itself more than twice. It’s no coincidence that the developed countries with the best paternal leave policies tend to have the lowest incidence of mental disorders (e.g.: 26.4 percent of people in the United States compared to 8.2 percent of people in Italy.) Of course more reasonable paternal leave doesn’t guarantee adaptation to the EDN persuasion of child rearing--a limitation of my numbers. A parent taking a 12 month leave may still execute cry-it-out sleep training, for example*. This means parent and clinician education is also in need of some attention and funding to have additional impact on child mental health. But longer paternal leave makes the EDN possible, and with an over $100 billion in net savings, there’s more than enough to enhance it in additional ways. *Please note, I'm not referring to allowing an older baby to self soothe for a few minutes of mild fussing, but rather an intense cry that is ignored and therefore triggers the baby's stress response system. (For a detailed explanation of the distinction, please see my post on Dr. Narvaez's blog.) High-Nurturing and the Gross National Product So why is our society, so afraid to invest in high-nurturing very early childcare? Because we fear it poses a threat to our productivity—to success. Those of us pleading for more support for families with young children can typically be found lobbying for a compromise: more attention to better parenting and less to the bottom line—a matter of values. When we define success more completely than only temporary productivity, the cost-benefit equation shifts. When we realize that success is most probable in a society made up of more healthy, functional individuals, our parameters broaden—perhaps even wide enough to support, not just breastfeeding, but the entire the EDN protocol. But recalibrating values is not the entire case to be made. Research shows that in the long-term, the same solution of several (longer maternity leave) to what Narvaez describes as undercare in our society would get more women in the workforce and increase national productivity, too. All over the globe, paid maternity leave policies have proven vital in boosting the likelihood that a new mother will return to work, and will put in more hours after she returns. The Women’s Movement Re-engineered Still, to factions of the women’s movement, the idea of intensive childcare biting an entire year’s progress off of women’s careers is a tenuous if not treasonous one. But here’s what they miss: longer maternity leave preserves a woman’s career in the long-run. Instead of giving up on careers altogether, because a non-paid six or 12 week leave is cruel and unreasonable, more women are likely to recover properly, adequately nurture their offspring—and then go back to their jobs. Japan recently put its money on it: Prime Minister Shinzo Abe increased Japan’s maternity leave policy with the goal of boosting the country’s GDP by 15 percent. Goldman Sachs revealed, in a paper in April of this year entitled "Women’s Work: Driving the Economy," that higher numbers of educated and skilled women in the labor force can boost competitiveness and generate growth with little incremental cost. Credit Suisse cites research suggested one reason more women with careers equals a healthier economy: Greater gender diversity in leadership improves communication and reduces corrosive competition among senior managers. Goldman’s earlier research showed that closing the gender gap in developed countries could push income per capita as much as 14 percent higher than their baseline projections by 2020, and as much as 20% higher by 2030. And longer—not shorter, or nonexistent—maternity leave is what will get us there. In return, all we ask is for is one year to give the next generation the nurturing it needs to thrive. It doesn’t have to be all or nothing and psychological evidence suggests that women want both: work and mothering. And so, by the way, do men. Equalizing the gender gap may lie squarely on fathers taking more time off with their babies. When men participate more in childcare in the first year, women's careers benefit and so does the economy. It's a simple investment: put in one year of leave, and get out 20 or 30 years of additional productivity. Economists predict that if American women worked at the same rates men did, U.S. GDP would be nine percent higher. More men fathering in the first year and more women working thereafter could turn the inequitable childcare tradition on its head—without denying the natural needs of babes. Extended parental leave for both parents, could keep even more women in the workforce, raise economic productivity, and give the women’s movement the genuine equality it seeks—in one fell swoop. Not to mention, it would allow dads to enjoy the deep fulfillment of a more hands on approach to raising their own children.
Regardless of what side of the “mommy wars” we think we’re on, looking at the issue through a biological and then economic lens can clarify the battleground: uniting us under one cause. The Evolution of Babies “She screamed like it was killing her,” as one mom client recounted (after trying to sleep train her baby according to the standard protocol of leaving her suddenly to cry alone at bedtime.) That’s because babies fear that it could, according to biological anthropology. (This is a scientific discipline currently ignored by the baby sleep trainers who are younger than it is.) Of course babies don’t understand the concept of actual death, but they do come programmed for nearly continuous physical contact because that’s precisely what ensured their survival for millions of years--babies equate isolation with danger. So when suddenly left alone, a young baby especially, can quickly spin into full panic mode—their instinct to survive is triggered. And even that can be okay. If that’s when we parents step in. When we offer the greatest gift to the survival-minded baby, soothing, the repeated process culminates into better mental development and better physical health (for soothing tips). When that baby’s panic is not calmed, however, as is prescribed in many sleep training methods, it sets into motion a developmental trajectory that’s quite the opposite of raising an independent, tough child. It sets the baby’s nervous system on high-alert (thus, our current anxiety epidemic). This high-stress state, when left alone, also contributes to a host of physical compromises, from immune to endocrine (hormones). Developmental neuroscience is beginning join biological anthropology to shine a light on the importance of listening to our babies. In fact, from an evolutionary neuropsychological perspective, babies seem to come programed with the need to feel not only safe, but valued. Feeling valued, which is also communicated each time we respond to our babies’ cries, boosts a host of mental health outcomes in the same way the cry-it-out practice increases risks for future anxiety. These innate safety and value needs point to the necessity of specific parenting practices in early life. Enter Darcia Narvaez, Ph.D, professor of psychology at Notre Dame. Her work has shown how getting these instinctual needs met well translates into a foundation for life-long well-being and better mental health. Narvaez has synthesized the latest research to pinpoint exactly what these baby-expected parenting practices are and their corresponding effects on early childhood development. Narvaez’s research indicates that the closer we get to the following these standards, the better, in terms of care that aligns with the natural, biological needs of our babies. She’s also coined a term to describe care that falls short of these evolutionary norms: “Undercare.” This serves to emphasize that we’re not referring to abuse and neglect, but something further down the spectrum that falls short of meeting the instinctual expectations of babies. Those standards of care are: a soothing birth, avoiding stress and pain as much as possible; consistent and positive responsiveness to babies cues/communication; multiple care-givers who are bonded to baby; breastfeeding (on demand and extended); lots of physical contact and affectionate touch; and creative free-play in nature with multiple-aged peers. Narveaz calls this paradigm the Evolved Developmental Niche (EDN) and it’s supported by concrete outcomes like, higher intelligence, better development of empathy, social aptitude, and attachment (itself protective against metal illness). The Financial & Economic Case for High-Nurturing Though numerous studies from across disciplines support the benefits of these ancient parenting practices, they don’t tend to mesh well with our modern cultural ideal of the “good baby”: one who dutifully plays with a light-up toy in her isolated playpen, quietly accepts a bottle every 3 hours from day one, and endures being dropped off with a rotating staff of strangers without a fuss. Of course quality daycare transitioned to gradually with respect to the individual baby’s comfort can make all the difference. But the reality is, many parents have to get back to work on a timeline that doesn’t allow for “gentle” or “comfortable” anything, let alone care anywhere close to the EDN. This makes aspects of modern parenting at odds with the natural needs of babies and this is where the future costs begin to accrue—not just in terms of the human condition, but also financially and economically. Case in point: short maternity and paternity leaves typically put adequate touch, responsiveness, and breastfeeding on the chopping block. Without a strong multiple-caregiver practice that includes night-care, a 12-week maternity leave—the federal requirement—can be punishing, for both parent and baby. At 12 weeks, maternal exhaustion is often at its peak, as the baby emerges from his fussiest period (2 to 12 weeks). Bonding has just begun for many of those parents with babies on the fussier side (let’s face it, it’s difficult to bond with a scream machine). The exhilaration of having a new baby has given way to an accumulated sleep deficient previously unmatched. Meanwhile, a 12 week-old baby’s social and emotional brain has just blasted off on its fastest growth-spurt ever, featuring structures and systems that form in direct response to human interaction with attachment figures. Critical periods for development that will never occur again are looming large. And at this most vulnerable and crucial time, the baby is to be handed off to institutionalized care during the day and left to cry-it-out alone at night? In light of healthy psychological development, Narvaez’s EDN begins to look less like a parenting manifesto and more like a societal mandate. In part 2 of this post, I’ll run the numbers to reveal why EDN-parenting pays dividends at the individual, corporate, and societal levels. What if this investment in very early child development improved the productivity of nations, saved billions on healthcare costs, and even better equalized the gender gap in the workplace? Here’s why it can.So, mommies unite (and daddies, too)! When we fight for a society that supports a high-nurturing babyhood, we all win.  All babies cry—some more than others. Parents I work with whose little ones fall into the "more than others" category would call that an understatement. They worry that something is wrong with their baby or that they're doing something wrong when the crying doesn't stop after a feed or goes on for hours in the evening. Once you've fed, burped, diapered, and checked for a rouge safety pin that must have somehow become lodged into your babies tender skin—even though you don't even use safety pins—the source of the crying can become quite a conundrum. Parents want to know why.
Theories on the cause of colic have shifted from a sort of infant version of irritable bowel syndrome (IBS) or gas, to neurological immaturity and nervous system overload. In my review of the research on colic and ongoing interviews with colic experts, I think one thing is clear, colic has different causes for different babies, but there are universally common characteristics of babyhood that show us what the usual suspects are. Some things, from biological to neurological, just go along with being a baby in those first few tumultuous months. Child psychiatrist and neuroscientist, Bruce Perry, MD, PhD, who I've found has one of the most profound understandings of how our brains develop, describes the extreme discontent babies suffer in the first months as resulting from the various rhythms of the brain not yet being synchronized. Eventually, Perry promises, "your baby's neurological rhythms will become synchronized like an orchestra." That's when the clouds part, the sun pierces your weary soul, and the angels sing. Your baby emerges as a real, responsive, connected person, rather than a crying machine. Until then . . . you gotta get your soothing game on! Another thing that seems clear, and at the same time enlightening, is that colic isn’t always colic—the diagnosis simply describes a symptom: crying for more than three hours a day, three times a week, for three weeks or more. This symptom can commonly be brought about when a baby's holding-time quota is not being met.This idea sprouted when I first read a blog post by Jay Gordon years ago in which he profoundly suggests that babies thought to be “colicky” simply need to be fed and held more. He describes working with parents on soothing skills in his pediatric practice and suddenly, their baby no longer fits the diagnostic criteria for colic. This dynamic is echoed in my work as well, especially with experienced mothers whose first babies were of a milder temperament. I would add that these babies often need more intensive help getting to sleep! This brings me to my gigantic colic caveat: All babies really are different. Some need far more soothing than others (and this is one of the simplest answers to why prolonged crying happens). Some are extremely more sensitive to being overtired (being awake too long between feeds), and some are actually gassy or have reflux. The approach I take with my coaching clients it to explore those usual-suspect causes directly. Through process of elimination and taking specific steps, we are able to drastically reduce the crying. Sometimes this improvement happens in just days, when the cause is the need for more soothing, for example, and sometimes it takes up to two weeks, like when there's a problem like reflux, allergies, or a combination of causes in play. Here is a checklist, step by step, you can go through yourself, if your little one (under four months) is suffering from seemingly inconsolable crying episodes, whether he’s been given a colic diagnosis or not: 1. Bring the crying to the attention of your baby’s doctor, not because your pediatrician will offer much help, unless they are of the rare Harvey Karp, MD, or Jay Gordon, MD variety, but because you want to first eliminate the possibility that there could be something physically, medically wrong that is causing your baby pain. (This is usually not the case, but a logical first step.) 2. Hold and carry your baby more both in general and just before the time the crying spells normally hit. Studies show, as Dr. Gordon observed, holding and carrying can drastically reduce prolonged crying for most, but not all, babies. 3. Reduce novel stimulation and simulate a womb-like environment. This is where Dr. Karp’s “5 Ss” as in The Happiest Baby on the Block, come in. Find a routine by using Karp’s combination of swaddling, shushing, side position, and swinging as a starting point and adding your own techniques if necessary through experimentation. Babies womb-experiences vary slightly, so their “calming reflex,” as Karp terms it, can be somewhat unique as well. Use this routine in a dark room with loud white noise to help your baby tune out the world and go to sleep. I'm also a big fan of Dr. Karp's Snoo Smart sleeper. Some attachment parenting purists worry that it will cause babies to not be held as much, but reality is parents must be able to put baby down to sleep some and for many babies, Snoo is the only thing that makes that possible, therefore it's a solution that protects the family's energy resources and sanity while providing biologically critical movement and sound stimulation. 4. Watch the clock if you have a fussy baby. This component of my approach was inspired by Mark Weissbluth, MD, author of Healthy Sleep Habits, Happy Child, who emphasizes the dramatic effect of "overtired"; he uses the term as a noun as if it's an entity (rightly so). This has lead me to a guiding belief that was later repeatedly validated by numerous clients as well as my own experience with my colicky daughter: these more sensitive babies are difficult if not impossible to read in terms of sleepiness. They will flip a switch on you and start wailing with none of the “sleepy signs” for which the baby sleep books tell you to watch. Take notes, and get ahead of the crying times by starting your soothing routine before the witching hour(s) hits. 5. If breastfeeding, try eliminating dairy (the most likely culprit), eggs, cruciferous vegetables, and wheat for two weeks (or ask your pediatrician for dietary guidelines). Breast milk is rarely the problem, but an allergy could be just the thing for your baby (especially suspect if the soothing and sleep stuff above didn’t make a difference). 6. If formula-feeding, ask your pediatrician for a hypo-allergenic formula and/or probiotic supplementation. Recent research, the latest of which was published just last month (Jan. 13 in the journal JAMA Pediatrics), has shown that colicky babies do have different flora (bacteria) in their intestines than non-colicky babies. In many cases, probiotic supplementation does reduce prolonged crying, reflux, and constipation, according to the study authors. This works presumably because it balances the intestinal flora, bringing just the comfort your little screamer needed. (I'm paraphrasing several studies and interviews here.) 7. With both bottle and breast, feed your baby in a slightly upright position and keep her upright and still for about 15 minutes after each feed. This will reduce acid reflux, which most babies have to some degree (diagnosed or not!). This is an easy thing to implement, but again, not usually the cause of colic. I’ve had clients with babies with diagnosed acid reflux but a funny thing happens after the three-month-mark (when the neurological rhythms calibrate and the need for a womb-like sanctuary dissipates). These babies with reflux still spit up all over the place after every feed, but now they laugh about it—it wasn’t the reflux that had caused their crying. One of the most useful revelations my research over the past three years has revealed is just how different one baby is from the next in terms of sensitivity. All babies are born immature (human brains are only 25 percent developed at birth). But, some babies are neurologically more sensitive to the discomforts which that underdevelopment can bring. There are universal truths. Most babies do instinctively desire a lot of holding and soothing in the first few months. But if you have a little one who seems to require constant holding, please don’t see it as a negative (even if this means they wail for 2.5 hours a day). It’s a challenge, to be sure, but your little touchy type may turn out to be more curious or more perceptive in later years. It’s just sad that quiet, easy babies are said to be “good babies.” There’s no good or bad in this. Your baby’s crying today is in part tied up in some aspects of her temperament, which is a neutral thing. It may be the very trait that underlies the things you’ll grow to treasure about her emerging personality in the years to come. As trying as this crying phase can be, it’s part of the wondrous journey with your one-of-a-kind little person. And like the challenge of giving birth to her, you’re in it together. Have more questions? Post them on Facebook and I will try to answer all!  Parents hate to hear their babies cry. They also need to get some sleep in order to be good parents. These two seemingly conflicting forces butt heads like enraged bulls throughout the parenting books and blogs. With everyone shouting at each other about how it should be done, it's easy to lose sight of the truly relevant questions: What is literally happening in baby’s brain when we leave her in a room to cry herself to sleep? (This is one popular solution to the ubiquitous sleep dilemma). It’s the answer to that question which holds the key to finding our way through the clashing advice and handling sleep challenges in the healthiest way possible for your unique baby.
One of the first subjects we tackle as little humans is the ever fascinating, cause and effect—What happens when I drop my food over the highchair? We come to count on cause and effect patterns that we learn, for a lifetime. Every time I go to Whole Foods with my kids, they hop into the “race car” shopping cart and we roll into the elevator. We want to go to the second floor for our snacks and salads. To cause that to happen, we push the elevator button, because we have learned repeatedly this causes the elevator to take us up to where we'll be rewarded with yummy (read: kale!) treats. One day, we push with confidence, but nothing happens. Bewildered, we push again, harder. We really don’t want to be down here in this elevator hungry, so we jab repeatedly at that second-floor button—still nothing. Next, two things happen and they are universal: One, we give up (feeling frustrated, we get out of the race car and take the stairs, and two, we learn that this elevator is unreliable! Pushing that button doesn't work like its supposed to. This little scenario is so universal in human and animal behavior that it has a name in the sciences. It’s termed, “extinction.” It may surprise you that the cry it out (in which baby is left alone to cry to sleep) method is, in fact, called the “total extinction” method by scientists who study such things (“controlled crying” methods are termed “partial extinction.”) The problem is, unlike in the elevator example, young babies are not able to take the stairs; they are stuck in a potential toxic avalanche of emotional “dysregulation.” As this blog post by Darcia Narvaez, PhD, pointedly outlines, this carries a host of legitimate concerns for neurological development. This is because contrary to popular myth, babies are unable to soothe themselves from extreme distress; they don’t have the brain function to do this, so extinction “teaches” them to self-soothe like tossing them in the ocean teaches them to swim. When they are tossed into extreme distress and comfort is withheld, the stress hormone cortisol actually destroys nerve connections in critical portions of an infant’s developing brain. It seems clear that extreme prolonged and repeated distress is cause for concern during the time the brain is growing and wiring exponentially more than it ever will again. But is it really that stressful? I’m just in the next room from little Junior's safe plush, CPSC-approved crib. There really is no cause for intense distress. We have to keep in mind that babies are operating primarily from their base-level survival instincts, which demand he keep his parent close to protect him, he actually doesn’t know he’s safe—he’s very likely afraid for his very life, as illogical as they may be to us, when he's suddenly left alone to sleep. This biological perspective puts the cry-it-out debate in a new light. Stress level vis-à-vis baby’s survival instinct and the neurological damage possible from it is one concern that’s been overlooked by advocates of the total extinction method. Now remember all that desperate jabbing of the button that we did at Whole Foods when the elevator failed to respond as expected? There’s a scientific name for that specific behavior, too: “an extinction burst.” This is when baby increases his cry to a higher, more desperate pitch when his trusted care-giver doesn’t respond to him. As a parent, you can practically hear the blood-pressure and stress hormones skyrocketing (or you can just look at the studies that have measured them). The extinction burst, before the behavior is extinguished, produces a different type of crying, far more severe than normal everyday crying. Mommy’s instinct is correct in feeling this level of distress needs attention. If you don't want extinction, the extinction burst is your cue to step in. This leads to another concern that rears its ugly head when we understand the process of extinction: What exactly are we are extinguishing? Is it the need for soothing, or the communication of that need? Scientists know that infant crying is communication, plain and simple. But researchers at the University of Texas took the understanding of crying communication to a new level when they set out to see what happened to stress levels of infant and their mothers when babies’ cry for help at sleep time went ignored. Inadvertently, this study busted the “teaching to sleep” myth used to prop up the cry it out method. Just as you’d expect, stress levels were extremely high when babies were left to cry, and mothers’ stress levels, of course, mirrored those of their screaming babes’. But after babies’ crying stopped (because their communication was not causing the desired effect) and they were officially "sleep trained," their stress levels remained elevated—they just didn’t express it. Did they learn that it's okay to go to sleep alone? Their little bodies suggest otherwise. But we already knew this communication suppression to be the true effect, because neglected infants found in Romanian orphanages didn’t cry at all, even though their discomfort was undeniable. John Medina, PhD, in his book, Brain Rules For Baby, says, “Indeed, you could walk into some of these hundred-bed orphanages and not hear a sound.” I'm not comparing a few days of crying it out to the orphanages level of neglect, but rather demonstrating what extinction is: stifling, not teaching. Given that building trust (reliability) and establishing communication, which are intertwined, are the hallmarks of healthy infant mental development, it seems unwise to use a method that compromises both. Babies come hard-wired to expect someone to respond to them; the elevator button is supposed to work! Aside from the concern over cortisol levels produced by crying it out, is it a good idea to teach baby that his primary attachment figure is unreliable, like that frustrating elevator? Is it advisable to condition him not to communicate his needs, which are based on powerful survival instincts? When I work with clients on baby sleep issues, we instead use an approach based on a brilliant psychological theory that originated in the 1930s: The Zone of Proximal Development, first asserted by the Russian scientist, Lev Vygotsky and validated and expanded over the following 80 decades. This allows me and the parents to create a sleep plan that pushes baby just enough to encourage real learning, without crossing a stress threshold that may break trust and dampened communication. We put baby in a sweet-spot that challenges him in just the right dose and frequency, based on his unique history, temperament, and age. It’s not cold-turkey; it’s not sink-or-swim; it’s not extinction; it’s actual teaching to sleep more independently. As for those cortisol levels of the mothers, after the babies stopped crying—they plummeted, no longer psychologically mirroring their still-distressed babies. The communication was broken, or as the researchers put it, “They no longer expressed behavioral distress during the sleep transition but their cortisol levels were elevated. The dissociation between infants' behavioral and physiological responses resulted in asynchrony in mothers' and infants' cortisol levels.” Parents need sleep and there are many things we can do to get it short of putting baby down and walking out that nursery door. Isn’t it better to approach sleep-training with respect for parent-infant synchrony, protection of developing communication, and assurance of lower stress levels for both mother and baby? Remember, they can’t walk out of the crib the way we can walk out of the elevator. During whatever period these desperate, intense-type cries are ignored, in their baby-perception, their very survival is at risk. For more on this topic, see my posts on Psychology Today with Dr. Darcia Narvaez. Please post sleep-training questions on my Facebook page and I'll coach you toward better nights without CIO.  Your adoration of Jr. is off the charts and you’re happy to jump at his every whimper, but if you also have a bit of “spoiling baby” mythology knocking around in your head, you’re not alone. These days, your pediatrician or mother-in-law may not tell you directly to let your baby cry himself to sleep (or they may tell you directly!) but more subtle anti-spoiling messages persist:
“Don’t go to your baby right away . . . let her fuss a little on her own for a few minutes before picking her up,” or “Don’t give her too much attention or she’ll always expect it.” These messages are still prolific, even if it’s just your stern Aunt Millie making you feel like a “softie." On a larger scale, the writer for perhaps the most-talked-about cover article of Time magazine of all time, "Are You Mom Enough? . . . " got it wrong when she approached her now famed profile piece based on the common assumption that attachment-style parenting is in opposition to developing independence in childhood. In fact, the research (e.g., Stein, J. A., & Newcomb, M. D. (1994) "Children's internalizing and externalizing behaviors and maternal health problems" Journal of Pediatric Psychology, 19(5), 571-593) shows the opposite: Healthy attachment results more often in nurturing the traits of independence and inner strength. (Mommies, I've scoured the research and have yet to find any science that supports the common notion that we can spoil little ones with attachment-inducing care!) To aim high on that healthy-attachment continuum, embrace your inner softie! Always comfort, hold, and soothe baby when she needs help getting back to her happy place. The science suggests in concert: The younger the baby, the more important this is. A major flaw in our cultural messaging surrounding being responsive to our babies is that much advice better fit for older toddlers gets applied to younger infants. Dr. Harvey Karp, author of The Happiest Baby on The Block series, stated it this way in a recent interview (with me), "Setting limits has absolutely no place in parenting babies under 6 months." Many specialists in the neuropsychology arena would move that bar closer to a year, while emphasizing that responding to distress is the key ingredient in optimum brain development (for at least the first 18 months). So just how responsive, doting, and attentive should we be? And how is the best balance struck between making your baby secure and fostering a little independence in the short term (as in, please go to sleep already!)? With toddlers and preschoolers we may push a bit for more independent sleep (without leaving them to cry it out). A great example is Dr. Karp's "patience stretching," (explained in his toddler book and DVD) an invaluable tool at the right developmental stage. But in babyhood, the fuse that launches baby into toxic distress isn't just short, it's virtually nonexistent. This is because the parts of the brain that regulate strong emotions are not fully formed. Once babies have been responded to consistently and lovingly for the first six months, they have built a certain level of trust in the world. Areas of the brain that determine social, emotional, and self-regulating capacities that were not there at birth, are more developed at this age (though they still have a lot of maturing and connecting up to do). Emotion-processing and stress-regulating genes have been turned on, according to positive emotional relations with caregivers, and six months of soothing has provided “scaffolding” (as the science set terms it) for the baby to begin to practice a little soothing on her own. At this point, a few minutes of protest crying to nudge baby toward more self-soothing may be okay in moderation, depending on the individual baby. (Babies develop at different rates and many continue to need parents’ help for several more months or years, at sleep times.) My standard approach with coaching clients is a no-cry one, but for certain individuals, factors like types of cries (because there's a genetic component to baby's sensitivity) and history and age of baby can neurologically and physiologically have very different effects. These factors can be gaged to determine how much, if any, we can safely push baby. This delicate approach is based in part on confirmation I received during email conversations with Dr. Allan Schore, a top expert on emotional and neurological development in the first year, and of course, after my studies of many textbooks and journal articles authored by him. "I agree with your position, and about the importance of age," Schore said when I ran my approach by him. In any case, it's developmentally imperative that baby gets the level of support she needs, despite what your pediatrician may sanction in the name of independence. The other vital key to surviving natural infant soothing needs involves practices that lay the ground work for future independent sleep. Not nursing/feeding completely to sleep every time and avoiding too strong an association between any one soothing technique and sleeping can help avoid the need for more aggressive sleep training later. Bottom line, any soothing style you embrace or specific sleep-plan you adopt must gel with your softie sensibilities . . . and your new, myth-busting knowledge of long term psychological development.  My two-year-old (pictured here at five months) lunges for my leg as we walk down a lush pathway of our neighborhood botanical gardens. "Whus dat?" she warily squeals as she jumps away from the moving object for a full body cling to mom. "It's just a stroller, Honey," I hear myself say, as the humor of our exchange hits me on so many levels (this one had a bright red canopy - perhaps the true cause for alarm). I could just think of some Attachment Parenting pundits who would have loved to have a video tape of that reaction to illustrate the purported evils of all things that hold babies (other than parents). It also struck me that my Gianna indeed hadn't been in a stroller for some time. She never would tolerate them for long and I'd end up carrying her anyway, so I guess I'd become unmotivated to lug the stroller out! But the parenting debate this hilarious moment brought to mind is no laughing matter. It represents a lot of needless divisiveness in the mommy realm.
While there is much to be said for the empirically supported importance of close physical contact, particularly for newborns (it literally regulates their breathing!), every thing in moderation (strollers and car seats, and playpens - oh my!) surely can apply. Rather than banishing strollers and other baby-holding paraphernalia, we mommies may be better served by focusing on what's really important in nurturing a healthy attachment. Just this week, the blogs are afire with another example of parenting zeal impeding into does-this-really-matter territory as Gisele Bundchen, supermodel mom and breastfeeding advocate, is widely criticized for having her eight-month-old daughter's ears pierced. In the interest of wrangling focus in the direction of things that really do matter, I'm going to highlight the three major practices scientifically-linked to building and nurturing a healthy attachment--the #1 predictor of infant mental health. 1. Affectionate Play. Play is bonding fuel for baby. Sharing pleasurable moments through excitement activates opioids in both play partners' brains. Along with dopaine and norepinephrine, these feel-good hormones help build and strengthen neural pathways that will make joy, playfulness, and positivity in general, more likely to be felt. In this way, play strengthens not only the immediate relationship, but paves the way for easier and more satisfying bonding in future relationships. Interactive, face-to-face play is neuro-psychologically beneficial from birth, helping certain right-brain social capacities to come online during the critical growth spurt happening in this hemisphere throughout the first 18 months. (Primary source: The Science of the Art of Psychotherapy by Allan N. Schore, PhD. 2012.) So, as long as we talk to stroller baby and point out funny scenery as we stroll by . . . 2. Regulation of emotional states. In the scientific community, the power of emotions is at a fever pitch. For babies, emotional regulation is even more important, both because they are in the process of developing soothing capacities and because their brains are in a tremendous growth spurt throughout the first year. When distressed or afraid, energy is robbed from brain growth while toxic stress hormones can even unhook neural connections that have already formed if negative emotions are prolonged. When a parent averts these negative effects and consistently soothes in response to emotional upsets, baby's bond with that parent is cemented while his brain is freed up to learn and explore in emotional safety. Baby trusts the attachment figure will be there for him, so he doesn't waste brain power worrying. (Primary sources: The Attachment Connection, by Ruth P Newton, PhD. 2008; and Why Love Matters, by Sue Gerhardt. 2004; "Effects of a Secure Attachment on Right Brain Development, Affect Regulation, and Infant Mental Health," by Allan N. Schore. 2001.) So unless baby cries inconsolably when placed in stroller . . . 3. Close physical contact. Ah, this is where those anti-stroller pundits may have a point. If we place baby in a stroller at times when he could be wrapped against our bodies in a cozy carrier, baby may be robbed of essential bonding-through-touch time. Touch really should be widely recognized as nourishment (it is in neurodevelopmental science). This is often why (my coaching clients are surprised to learn) babies wake in the night even after all other reasons have been eliminated; they need a refueling of physical contact. My favorite scientist for this topic is currently Tiffany Field, PhD of the Touch Research Institute. There's no doubt, touch and holding communicates love and safety, which I believe are one and the same in early babyhood. But perhaps if we co-sleep at night and give lots of cuddles around the clock, not to mention the proven attachment-promoting effects of breastfeeding in and of itself (Thanks, Gisele Bundchen!), we can indulge in a stroll and still meet baby's touch quota. In any case, shouldn't we mommies focus on the essence of parenting practices that really contribute to attachment rather than on the specific practices themselves . . . or the apparatus involved?  Drop off play dates? Do them. Postpartum doulas? Book them. As communities across the country strive to be more connected, environmentally-conscious, and family-friendly, an ancient parenting style may be poised for a comeback. And it may be the only truly sustainable model. Drop off play dates? Do them. Postpartum doulas? Book them. As communities across the country strive to be more connected, environmentally-conscious, and family-friendly, an ancient parenting style may be poised for a comeback. And it may be the only truly sustainable model. Whether you subscribe to “Attachment Parenting” or not, this powerful practice crosses the parenting-style divide. It’s called “alloparenting” in the sciences; to us mommies, it translates to something we desperately need: the helping hands of others. And for the attachment-science-leaning crowd, we need helping hands with a lot of heart, too.
As a human species, we were never designed to go it alone in the baby-rearing department and yet, that is exactly the expectation our modern culture has recently (in evolutionary terms) upheld. The baby is typically the sole responsibility of the nuclear family, and really, just the parents . . . and many times, just one parent. This is an enormous diversion from the norm when considering most of human history. If you’ve been that one and only caregiver for an infant, the necessity to bring others into the mix is quickly clear. But how exactly do we modern parents meet those unrelenting newborn needs, short of hiring a full time nanny and housekeeping staff? The degree to which baby needs us to embrace the help of others has been less obvious. But decades of developmental research clearly demonstrate the importance of sensitive, emotionally responsive care giving, especially in the first year or so of a baby’s life, and more recent neuroscience is confirming this. Allan N. Schore, PhD, who is a top authority on how emotional relationships in infancy shape the human brain for life, says, “During critical periods, brain growth is exquisitely susceptible to adverse environmental factors such as dysregulating interpersonal affective experiences . . . which negatively impact infant mental health.” This is not one expert opinion, but the conclusion of a thought leader who specializes in synthesizing the latest findings from studies across disciplines like neuropsychology and developmental neuroscience. (If you’d like a thorough breakdown of the plethora of research available to back up this line of thinking, check out a textbook or two Schore has authored, like The Science of the Art of Psychotherapy or most recently, Evolution, Early Experience and Human Development.) The critical periods Schore refers to happen disproportionately in the first 18 months of life. During the first two years of your baby’s life, she will form all of her brain structures and her brain volume will grow from 25 percent of its final size to 80 percent. The fact that the brain is so unfinished at birth, forms so incredibly quickly and directly in response to “other brains” as Dr. Schore astutely states, makes a biological basis for Alloparenting undeniable. Baby simply needs more attention than modern environments are able to give. One reason this is true, is that those “dysregulating interpersonal affective experiences” (translation: emotional experiences related to others, or lack of others, which throw the maturing nervous system out of balance) that Schore cautions against are a constant threat in the reality of modern life with a baby, especially in the first three to four months. While not a popular assertion in the mainstream, science does seem to suggest that someone has to be hands-on and synced in virtually around the clock in order to give the average baby what she needs for optimum brain development. And yet, a mother is just one person (or father; I’m assuming here that one parent is out being the breadwinner). How can one person provide all the regulation, loving input, affection and holding a completely helpless, unfinished little person needs 24/7 when she or he has a zillion other responsibilities? Part of the answer has to be that those needs be met by more than one—some modern form of alloparenting. Anthropological evidence shows that, even before mom’s role expanded to include board meetings, financial reports and the PTA, she needed a great deal of help, especially in the first year. Our human ancestors parented in groups and many experts, like anthropologist, Sarah Blaffer Hrdy, PhD, believe the practice of engaging multiple caregivers was a key to the survival of our species. It may also have, in part, allowed for our bigger brains, heightened intelligence, and social complexity—all good things. And yet, our modern culture in many ways has strayed from this essential component of human well-being and perhaps even survival. Sure we have daycare to take over after mom goes to work, but there are empirically based concerns about the mental health impact of daycare in the first year, primarily for the emotional-regulation reasons Schore and others voice. (There are negative correlations.) Add to that, longitudinal research on neglected babies orphaned at birth suggests that by the tender age of four months, the human baby must establish a trust in the world through bonding with another person or be at risk for future mental health disorders. Yet, the first three to four months can be exactly when many modern mothers feel most isolated and exhausted, often interfering with her ability to regulate and bond. The postpartum depression rates for both mothers and fathers (spirally upwards of 20 percent) suggest the impossibility that has been perpetuated as “work-life balance.” Could alloparenting be the missing key? It’s a question that goes beyond the “mommy wars” over working outside the home or practicing a certain parenting style. The current neuroscience strongly suggests that a “high-nurturing” and “attuned” caregiver who regulates baby’s emotions is the most important component of optimum brain development, whether mom goes to the office or not. Sensitive care-giving with lots of positive face-to-face interaction, scientists are seeing, is far more influential than whether baby goes in the crib at night and the stroller during the day (unless, of course, he’s crying the whole time). These are tricky matters, which I’m not dismissing at all, as you’ll see in future blog posts. The point is we need to focus on the essence of parenting that is good for babies and then figure out how to make it work in reality. Often culture places this the other way around. Practices that transcend the mommy-wars-divide to deliver optimum infant health is going to be a major theme of this blog. For me, that has meant choosing caregivers who bond with my babies. It has meant hanging around the preschool longer than I was welcome until my little guy stopped clinging and started playing, rather than having him peeled off of me by a stranger; it has even meant not working for a period of time. What have you done or are you doing to ensure your baby’s emotional regulation? Let’s share strategies and ideas, especially when it comes to rallying the support of others to get our babies the attention they need to thrive. With grandparents (the most common alloparents traditionally) suffering failing health at younger ages and extended families facing geographical distance, many of us have to get creative. We have to bring in substitute family to fill the biologically based void in baby care—the void of others. Flexible work schedules, extended maternity and paternity leave are probably needed, I admit, but alloparenting is not to be overlooked in closing the gap between what baby needs and what parents can give. World-renowned biological anthropologist, James McKenna, PhD, who has studied the early motherhood era for decades, became fascinated early in his prolific career by a question that has likely crossed most moms’ minds at some point: “What is it that makes caring for a baby so difficult for some and fairly breezy for others?” (I’m paraphrasing the question.) The single biggest factor, McKenna concluded, in determining a thriving newborn chapter, was given to me, without hesitation, in one word: “alloparenting.” I would add one adjective that would make it healthier too, based on what I’ve learned about brain development from Schore and others: emotionally-regulating alloparenting. It’s a tall order, and yet, there it is. We can’t deny it; how are we going to meet it? |


Archives
August 2016
Categories
All
The Others Effect:
Author
Angela Braden is a journalist, researcher, and parent educator devoted to early parenting based on baby brain development. This blog explores what science shows we can do as parents to give our little ones the best foundations for life. |

 RSS Feed
RSS Feed
